
UPDATE – Please view our Goldilocks/SWIM information page here for up to date info, a photo gallery, and more!
Reconstructing a normal anatomic chest contour post-mastectomy using a new plastic surgery technique without implants or distant tissue donor sites
As patient demand grows for high quality, aesthetically pleasing flat mastectomy closures, cutting edge surgical techniques will be part of the conversation. Today we discuss a new technique called the “Goldilocks mastectomy,” or SWIM. This option, while not currently available to most patients, focuses specifically on maximizing cosmesis for patients having mastectomies without traditional reconstruction.
It’s important to note that because this is a new procedure, there is no long term data on its safety from an oncology perspective. The surgeons who offer it say that its risks are similar to that of a skin-sparing mastectomy. We look forward to seeing data on this.
Why Not Use Traditional Breast Reconstruction?
Traditional breast reconstruction involves additional risk beyond simple mastectomy and can impair function. Patients who reject traditional breast reconstruction are often motivated by wanting to preserve form and function for the rest of their bodies.
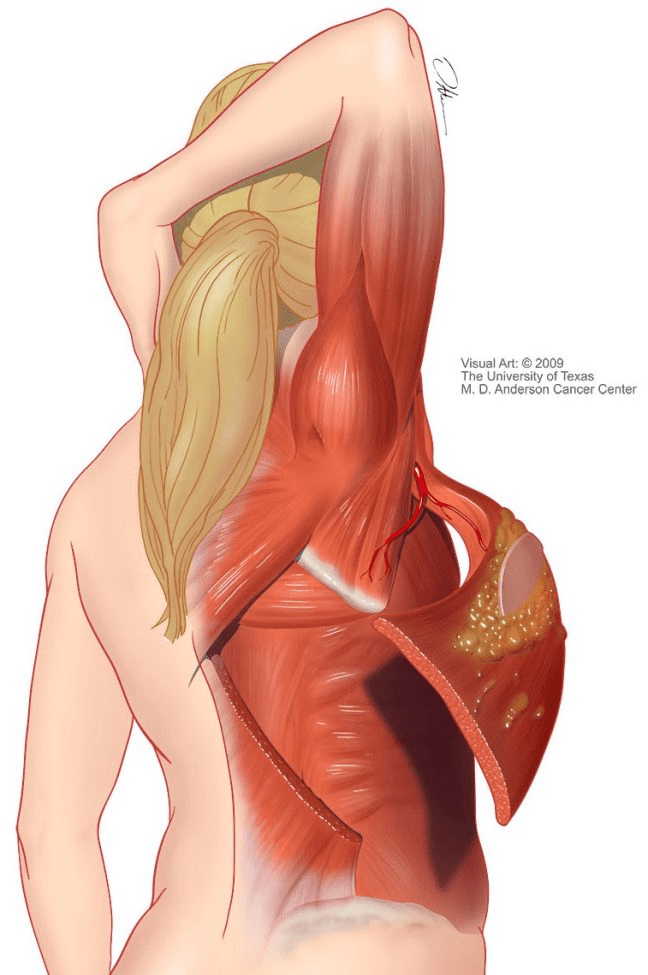


Rejection of autologous flap reconstruction, for example, avoids a second surgical wound that may compromise recovery time and/or function – especially in the case of muscle tissue transfer, i.e., LD (Figure 1) and TRAM flaps (Figure 2). Rejection of submuscular implant reconstruction avoids damage to the pectoral muscle that can impair function (this muscle is partially detached from the ribs to accommodate the device) (Figure 3).
These patients are also motivated by minimizing their exposure to additional surgeries beyond the original mastectomy, and traditional reconstruction almost always involves multiple surgeries.
Flat IS Reconstructive – Not Cosmetic
ALL patients care about their cosmetic result. But cosmesis for patients going flat has historically been devalued or outright ignored. A common misconception about these patients is that they “don’t care about how their body looks.” This notion is rooted in historical sexism and sexual objectification of the female body.
The truth is that these patients have made an affirmative, informed decision. They have weighed their options and are simply not willing to shoulder the risk burden presented by traditional breast reconstruction in order to achieve an artificial breast mound. So, they proceed with the default reconstructive option: no reconstruction, or going flat.
In terms of cosmesis, patients going flat report desiring a smooth, flat (not concave) result with the original breast contour removed to the greatest extent possible. The ideal resulting contour would approximate that of the prepubescent female chest – a reconstruction of a normal anatomical structure that falls squarely into “reconstructive surgery” territory… not cosmetic.

Unfortunately, many patients going flat are left with results that are nowhere near smooth or flat – concavity (which is largely unavoidable with traditional techniques), lumps, sagging excess skin (“in case you change your mind” about implant reconstruction (Figure 6)), redundant fatty tissue, dog ears, wrinkled/puckered incisions, and asymmetry (Figure 4).
It seems that until very recently, no one has thought to ask the patients making this choice the simple question, “what DO you want your chest to look like post-mastectomy?”
Traditional surgical techniques to remove all redundant (excess) tissue and create a smooth contour go a long way to producing results patients can live with. But even with a dedicated and highly skilled oncoplastic surgeon, and/or plastic surgeon using traditional techniques, patients can be left with significant concavity – the appearance of being “scooped out.” Concavity is currently addressed with fat grafting, which means additional surgeries, pain and bruising at the donor site, uncertain cosmetic results, and sometimes produces hard lumps (fat necrosis) which can be distressing to patients.
The New Middle Way? Using Local Tissues to Contour
What if there was a “middle way”? What if patients could choose reconstruction of a flat/convex structure or very small breast mound, with a moderately longer anesthesia burden, but without comprising any other part of their body – and without the need for multiple surgeries?
Plastic surgery techniques for breast mound reconstruction have advanced in recent years, and many of these techniques can be adapted to improve cosmesis for patients who choose to forgo traditional reconstruction. Thanks to the pioneering work of Dr. Grace Ma, Dr. Heather Richardson, and Dr. Lisa Cassileth, some patients* can now choose this “middle way” – it’s called the SWIM, or “Goldilocks mastectomy.” In this procedure, excess fat and skin adjacent to the breast tissue that has historically been discarded is instead repurposed to contour – or reshape – the mastectomy site. And it can be done in one surgery.

In the SWIM (Skin-sparing Wise-pattern Internal Mammary Perforator) procedure, a skin-sparing mastectomy is first performed to remove the breast tissue. Then, excess healthy skin and fat in the local area are processed (de-epithelialized) and arranged to create “padding.” The mastectomy flap is then closed around the padding to create varying sizes of reconstructed convex structures.
The size of the resulting structure will depend on the amount of healthy tissue that was available. Larger breasted patients may be able to achieve a mound that is easily recognizable as a female breast (Figures 7 and 8 represent patients who elected SWIM at their initial mastectomy surgery). Smaller breasted patients or patients pursuing revision surgery (after a poor initial cosmetic result, or during/after explant – so may not have had the nipple preserved) may end up with a flat or only slightly convex contour (Figure 5). You can find more Goldilocks images at Dr. Grace Ma’s site.


Consider the time, risk and expense of traditional breast mound reconstruction: up to six to twelve hours under anesthesia at the initial procedure, up to 9 (or more) surgeries over a period of a year or so, upwards of a 30% complication rate, and hundreds of thousands of dollars expended.** This burden has clearly been deemed acceptable by surgeons, patients, and the insurance companies who are footing the vast majority of the bill. In this framework, is it unreasonable to consider that patients going flat should be able to access surgical procedures involving a fraction of these outlays, in order to achieve a cosmetic result that they can live with?
Patients going flat deserve equal care and consideration for reconstruction of an anatomically normal chest contour.
The goal is not perfection – the goal is parity. It’s time to ensure that all mastectomy patients receive the respect, care and consideration they deserve, to achieve a surgical result that they can live with – regardless of their surgical preferences.
See below for references, glossary, a list of surgeons who currently offer SWIM, and suggestions for further reading.
Questions or comments? NotPuttingonaShirt@gmail.com
References
* it should be noted that not all patients will be good candidates for a given surgical procedure
**The Number of Operations The Number of Operations Required for Completing Breast Reconstruction , Eom, J.S., Plast Reconstr Surg Glob Open. 2014 Oct; 2(10): e242
Comparison of 2-Year Complication Rates Among Common Techniques for Postmastectomy Breast Reconstruction , Bennett, K.G.,
Financial Impact of Breast Reconstruction an Academic Surgical Practice, Alderman, A.K., Plast Reconstr Surg. 2009 May; 123(5): 1408–1413
Glossary
autologous flap reconstruction = use of the patient’s own tissues to recreate a breast mound
cosmesis = aesthetic appearance
chest contour = topography or three-dimensional shape of the chest
de-epithelialization = removal of the epidermis without compromising the vascularity of the dermis, to allow the rearranged tissue to heal properly
Goldilocks mastectomy = SWIM flap (below)
oncoplastic reduction = a procedure which combines lumpectomy with rearrangement of the remaining tissues to create a breast mound – similar to Goldilocks mastectomy but doesn’t remove all the breast tissue
SWIM Flap = Skin-sparing Wise-pattern Internal Mammary perforator. A new plastic surgery technique in which the extra local skin and fat of the original breast contour left over after mastectomy is folded to create a smaller, reduced breast mound. Also called “Goldilocks mastectomy.” Skin sparing is employed when possible at the original mastectomy to preserve the nipple and/or maximize cosmesis.
Who performs these procedures?
At present, only a small number of surgeons advertise that they offer these services, including but not limited to:
| Dr. Marguerite Barnett Sarasota Institute of Plastic Surgery Sarasota, FL https://drmbarnett.comDr. Lisa Cassileth Cassileth Plastic Surgery Beverly Hills, CA https://www.drcassileth.comDr. Lisa Jewell Surgery Center of South Bay Torrance, CA https://www.surgerycentersouthbay.com
Dr. Sendia Kim |
Dr. Grace Ma Peachtree Plastic Surgery Atlanta, GA http://www.peachtreeplasticsurgery.comDr. Heather Richardson Bedford Breast Center Beverly Hills, CA https://www.bedfordbreastcenter.comDr. Shannon Tierney Swedish Hospital Seattle, WA |
Further Reading:
SWIM Flap Breast Reconstruction – Cassileth Plastic Surgery
Goldilocks Mastectomy – The Bedford Breast Center
Goldilocks Mastectomy with Bilateral In Situ Nipple Preservation Via Dermal Pedicle, Richardson, H. et. al., Plast Reconstr Surg Glob Open. 2018 Apr; 6(4)
The Goldilocks Mastectomy, Richardson, H., Ma., G., Int J Surg. 2012;10(9):522-6
Outcomes Analysis of Goldilocks Mastectomy and Breast Reconstruction: The Mayo Clinic Experience, Oliver, J. et. al., Plast Reconstr Surg Glob Open. 2018 Apr; 6(4 Suppl): 61-62
It’s important for patients to be informed about all the available options for mastectomy closure and reconstruction, and to discuss the risks and benefits of each option with their healthcare provider. While the Goldilocks mastectomy technique may be a promising option for some patients, it’s crucial to keep in mind that it’s still a new procedure, and more data is needed to evaluate its safety and effectiveness. Thank you for sharing this.